










Heart failure (HF) is a common condition with significant morbidity and mortality. One of the therapeutic options for advanced management of patients with HF with reduced or preserved left ventricular ejection fraction (HFrEF or HfpEF, respectively) is CRT. In a selected population of candidates, it improves symptoms, quality of life, and prognosis. However, not all patients respond favourably to CRT, which indicates that there are unsolved issues in accurate patient selection and the proper delivery of CRT.1 Several characteristics predict improvement in morbidity and mortality, and the extent of reverse remodelling is one of the most important mechanisms of action of CRT. Of the clinical parameters, QRS duration is always used as an outcome parameter in all available trials, but consensus has not been reached regarding the optimal ECG-based criteria for patient selection for a CRT device.
The strategy for CRT device optimisation also remains challenging. The available methods include echocardiography, ECG QRS-based assessment, invasive haemodynamic measurements, and/or non-invasive cardiac mapping.2 Among others, ECG imaging (ECGI) may be a comprehensive tool for measuring ventricular electrical dyssynchrony.3–5 However, the results are fragmentary and have not been summarised. This paper reviews the current knowledge on non-invasive ECG mapping methods for patient selection, left ventricular (LV) lead positioning, and optimisation of CRT programming, to determine the major trends and future perspectives for the application of these methods in CRT patients.
Given that the body surface potential mapping (BSPM) and ECGI methods are used mostly in the research field rather than in clinical settings, no standardised terminology concerning the specification of approaches exists. For this review, the methods related to the analysis and interpretation of body surface multi-lead ECG are referred to as BSPM. Techniques involved in the reconstruction of myocardial electrical potentials using body surface ECGs are termed ECGI.
Methods
A systematic literature review was carried out to evaluate the available clinical evidence regarding non-invasive cardiac mapping methods for patient selection, lead placement, and optimisation of CRT programming. The preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement was used as a basis for this review.6
In this review, we included randomised controlled trials and observational studies, such as cohort studies or case–control studies. Conference abstracts, letters and case reports were excluded. To cover all available evidence, we did not use any publication date restrictions.
The search was conducted using MEDLINE (through PubMed), Web of Science and Scopus databases. No limits were applied to language and foreign papers were translated. The reference lists of all included publications were checked to identify additional relevant studies. We also examined any relevant retraction statements and errata for the included studies.
The search terms included ‘CRT’, ‘BSPM’, ‘ECGI’, ‘electrocardiographic mapping (ECM)’, ‘congestive HF’, ‘HFrEF’, and various combinations of these terms. The full search strategies are given in the Supplementary Material.
The selected review publications were used to identify other publications not covered by our search. From the original studies included in the qualitative analysis, we extracted the following characteristics for each included study: participants (number of participants, target population); BSPM type (ECGI or simple BSPM); and BSPM parameters (definition and findings).
Duplicate articles were identified and excluded. Title and abstract screening for eligibility was performed by two reviewers independently. The full text of citations judged as potentially eligible was retrieved and screened in a blinded manner. The disagreement between the reviewers was then resolved by discussion or, if required, with the help of a third independent reviewer.
Results
Search Results
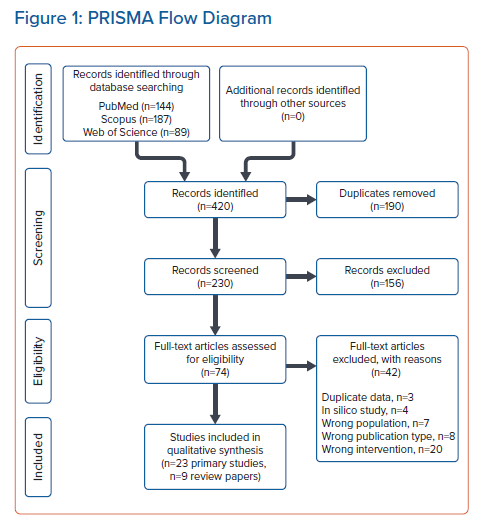
The literature search was performed on 21 January 2020. In total, 420 publications were identified in the main sources (PubMed, Scopus, and Web of Science). After the title and abstract screening, 156 records were excluded. The full text of 74 records was assessed for eligibility, and 23 original studies met the inclusion criteria. The procedure for selecting publications is shown in the PRISMA diagram (Figure 1).
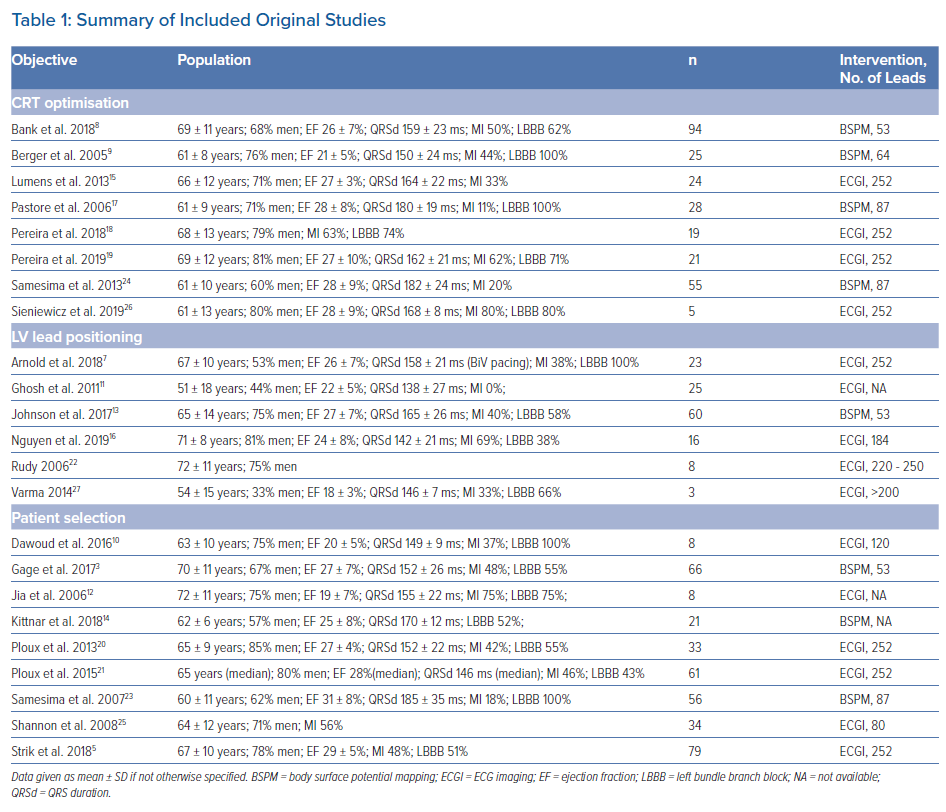
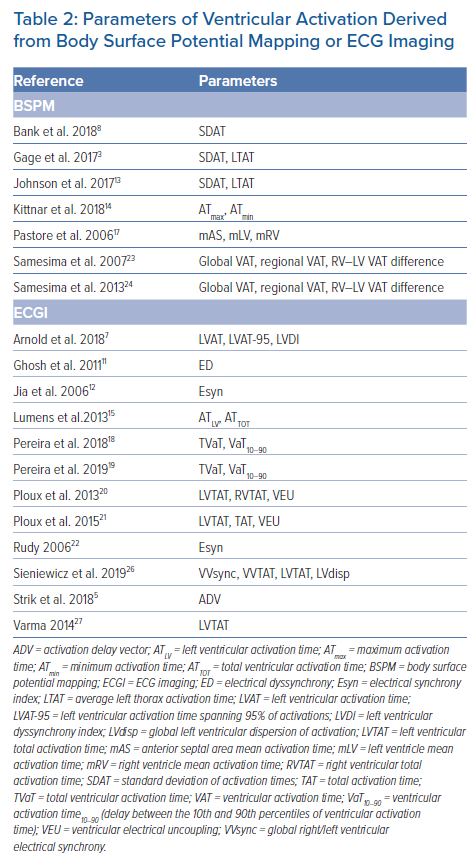
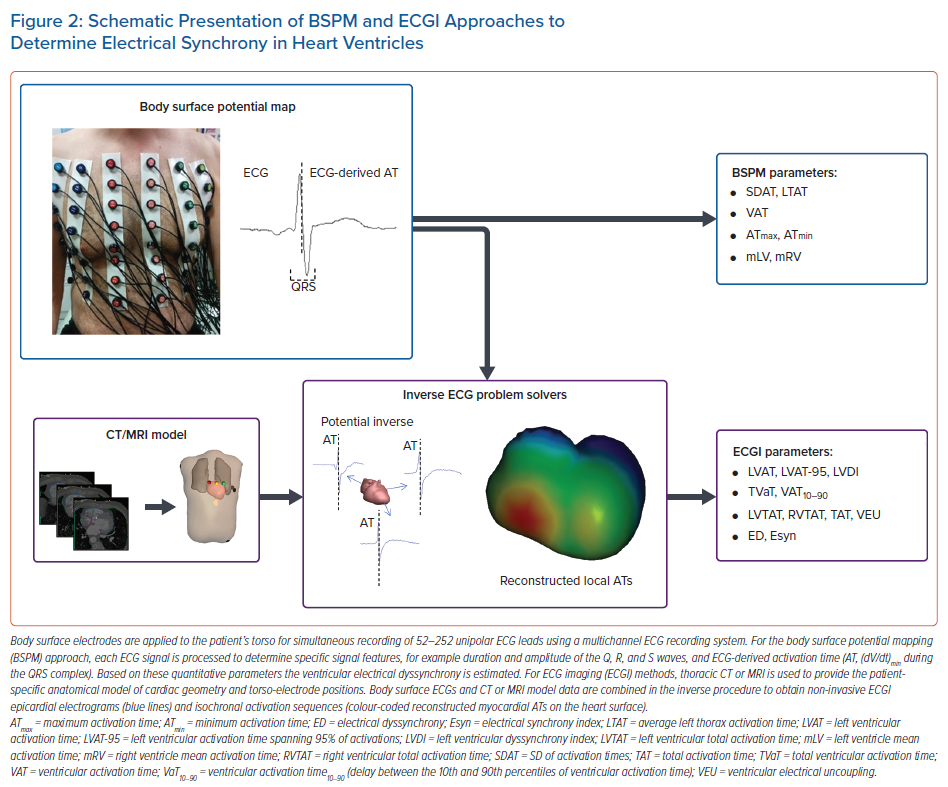
Table 1 summarises the 23 selected original studies in the population, intervention, control and outcomes (PICO) format.3,5,7–27 They include both BSPM (n=8) and ECGI methods (n=15). The median number of body surface leads used for ECGI was higher than for BSPM techniques (252 [IQR 192–252] versus 64 [IQR 53–87], respectively, p<0.0001). Non-invasive cardiac mapping approaches were applied in patients with CRT in several scenarios: the prediction of CRT response and patient selection; the selection of optimal LV pacing site; and the optimisation of CRT programming. Quantitative parameters of ventricular depolarisation are listed in Table 2. BSPM characteristics of depolarisation were mostly based on the detection of activation time, defined as the minimum of the first derivative of potential with respect to time during the QRS complex in unipolar body surface ECG leads. Parameters of ventricular activation obtained from reconstructed epicardial electrical potentials using ECGI techniques included local characteristics of ventricular depolarisation such as LV activation time, the interventricular difference in activation time, and intraventricular activation time distribution (Figure 2).
Patient Selection for CRT
Current European Society of Cardiology guidelines approve CRT as an indication for patients with symptomatic HFrEF and intraventricular conduction abnormality, especially QRS duration >150 ms and left bundle branch block (LBBB) morphology. In contrast, patients with QRS duration <120–130 ms are not indicated for CRT, due to a low success rate and possible worsening of HF.21,28
Assessment of electrical dyssynchrony is important for the accurate identification of appropriate CRT candidates. Although QRS duration is used as an indirect measure of dyssynchrony, some studies noted a weak correlation between QRS duration and mechanical dyssynchrony.29,30 BSPM and ECGI approaches have been applied in clinical studies to develop reliable parameters of ventricular activation for assessment of the CRT effects (Table 2).
BSPM-based Selection Criteria
BSPM-derived activation time (AT) is the duration between the QRS complex onset and the steepest negative slope of the QRS complex.3 This can then be visualised as body surface isochronal maps of ATs. The isochronal maps of ATs have been obtained using BSPM with 53 ECG leads to assess the changes in electrical dyssynchrony in patients with CRT. Quantitative metrics of dyssynchrony such as the standard deviation of activation times (SDAT) and average left thorax activation time (LTAT) have been suggested. Patients with native SDAT ≥35 ms and QRS duration ≥120 ms had significant reverse LV remodelling (improvement in left ventricular ejection fraction [LVEF] and decrease in end-systolic volume), thus both parameters have been suggested as predictors of CRT response.3 The longest activation time (ATmax) detected in any of 123 unipolar chest leads, served as a reliable dyssynchrony marker to predict CRT outcome.14 The right ventricular to left ventricular (RV–LV) activation gradient was identified through measures of QRS durations in 87-lead BSPM. It was suggested that an RV–LV activation gradient <20 ms during biventricular pacing could identify patients with improved functional class after CRT.23
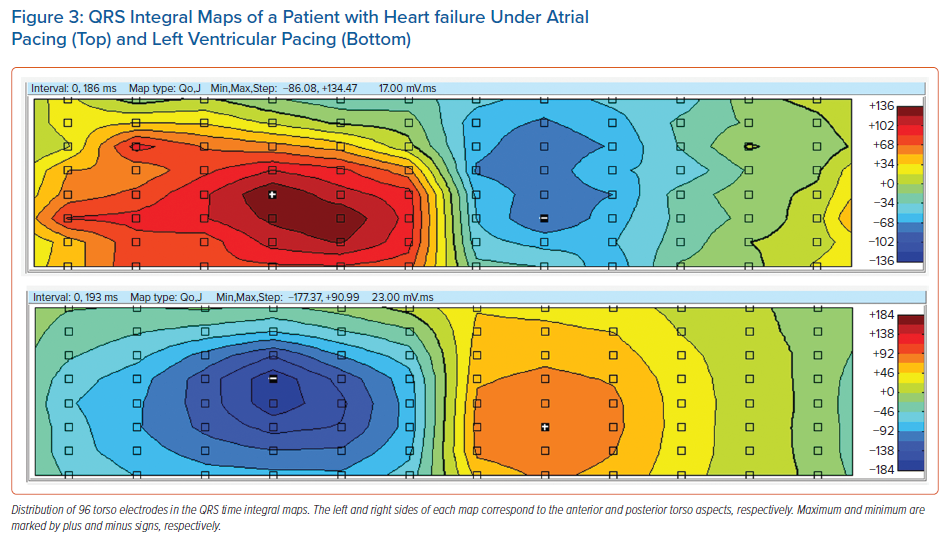
In our pilot study, an analysis of ventricular depolarisation was performed during different pacing configurations in selected patients using the QRS integral maps produced from a 96-lead mapping system (unpublished data). A 46-year-old patient with a history of post-myocarditis cardiomyopathy, LBBB (QRS 172 ms) and progressive LV dysfunction (LVEF 30%) underwent permanent CRT defibrillator (CRT-D) implantation in 2019, leading to reverse remodelling 6 months after CRT-D implantation (improvement of LVEF to 45%). The distribution of positive and negative time integrals correlated with the acute haemodynamic response to the different pacing configurations. Obtained time integral maps of the QRS complex reflected the improvement in LVEF during LV pacing compared with atrial pacing (Figure 3).
ECGI-based Selection Criteria
In patients with LBBB and non-specific intraventricular conduction disturbance (NICD), an ECGI-derived index of electrical dyssynchrony, ventricular electric uncoupling (VEU), defined as the difference between the mean epicardial LV and RV activation times, served as a significant predictor of response to CRT. It was concluded that in consecutive CRT candidates with QRS duration ≥120 ms, VEU is a more reliable predictor of clinical CRT response than QRS duration or the presence of LBBB.20 Supporting data were obtained in the study in which VEU was calculated at baseline and during biventricular pacing to assess the resynchronising effect in relation to the underlying electrical substrate. Responders had higher baseline VEU and more intensive reduction of VEU in response to biventricular pacing than did non-responders.21
Given that VEU represents the impairment of ventricular depolarisation only with regard to time, an activation delay vector (ADV) adds an additional parameter: a direction in space. This parameter represents a comprehensive electrical substrate, such that patients may have a similar direction of activation delay but a great difference in its magnitude. This parameter might be used to determine right-to-left activation delay and identify responders.5
Electrical synchrony of ventricles was assessed using isochronal activation maps obtained with the ECGI technique. The interventricular synchrony index, Esyn (the difference between activation times in the RV and LV), for estimation of electrical synchrony, however, did not always correlate with clinical improvement.12 In that case, a non-invasive ECGI approach for reconstruction of epicardial ventricular activation was then applied, in combination with cardiac magnetic resonance used for mechanical imaging of dyssynchrony in the LV. Electromechanical dissociation has been suggested as a marker of reduced response to CRT.10
Spatiotemporal myocardial activation maps were constructed using the ECGI method in patients with wide QRS complex before CRT. The different patterns of myocardial activation described suggested an association between electrophysiological pattern and the effect of CRT.25
In summary, the most promising predictors of response to CRT appear to be SDAT and LTAT, parameters that can be derived from BSPM, without the need for 3D imaging. These parameters are easy to obtain and analyse.
LV Lead Placement
The degree of cardiac resynchronisation response is influenced by many factors, of which the position of the LV lead on the heart is an important one. Many strategies have been used to optimise LV lead placement. Some of them use QLV interval, that is, the time between Q onset on the ECG and local depolarisation at the LV electrode, as measured during implantation, to determine the site of the latest activation. Other strategies involve echocardiography or MRI to evaluate the proximity of the lead to the site of maximal mechanical dyssynchrony.
BSPM-based LV Lead Placement
More recently, BSPM has been suggested as another alternative for LV lead positioning.2,13 The pacing site with the greatest decrease in SDAT and LTAT has been shown to have a strong correlation with the acute haemodynamic response measured invasively.13
ECGI-based LV Lead Placement
In patients with a quadripolar LV lead, ECGI visualisation of endocardial and epicardial activation was applied to identify the optimal area for pacing, that is, the site with the shortest total activation duration of both ventricles.27,31 ECGI isochronal maps of epicardial ventricular depolarisation also enabled the guidance of LV lead placement for improved clinical outcome.22 Another study integrated ECGI with CT angiography and cardiac magnetic resonance to develop the ‘CRT roadmap’, which provides data on scar localisation, epicardial activation sequence, and coronary venous anatomy. This CRT roadmap was suggested to be a reliable tool to guide LV lead placement.16
In some cases, LV lead placement is suboptimal due to unfavourable anatomy of the coronary venous system, and the response to CRT may be inferior.32 Recently, His bundle pacing (HBP) has emerged as an alternative to CRT. With the help of ECGI, it was established that HBP reduced LV activation time and LV dyssynchrony index (LVDI) more than twofold compared with biventricular pacing.7,11 The His-SYNC (His Bundle Pacing versus Coronary Sinus Pacing for Cardiac Resynchronisation Therapy) pilot trial was an investigator-initiated, prospective, randomised controlled study that demonstrated that there were no significant improvements in ECG or echocardiographic parameters compared with biventricular pacing-CRT.33
Optimisation of CRT Programming
LV pacing and biventricular pacing have a similar, positive effect on the haemodynamic function of patients with HF, while RV pacing alone is highly ineffective.12,17,22,34
BSPM-based CRT Optimisation
BSPM parameters such as SDAT can be useful for both LV pacing and biventricular pacing programming.8 CRT programmed at baseline settings can reduce dyssynchrony by up to 20%. This improvement is greater in the LBBB group of patients with wide QRS, and is lacking in the non-LBBB group. However, individualised and optimised settings based on BSPM parameters, such as SDAT, can further improve ventricular activation time by 46%, compared with standard pacing settings.3 SDAT reduction ≥10% was a significant predictor of improved ejection fraction and LV end-systolic volume response. With CRT optimisation, it is possible to achieve twofold improvement in electrical synchrony, regardless of patient baseline characteristics.8 Another BSPM approach based on measurement of QRS duration in 87 body surface unipolar leads showed that regional activation time in the RV increased in biventricular pacing, but it was compensated for by an even greater decrease in activation time in the LV, therefore the effect of CRT could be optimised by decreasing the inter-regional RV–LV gradients.23,24 In addition, BSPM parameters of ventricular repolarisation dispersion such as Tpeak–Tend interval, Tpeak–Tend integral, and T wave amplitude were reduced compared with sinus rhythm under biventricular pacing, whereas RV or LV pacing resulted in increased dispersion of repolarisation.9
ECGI-based CRT Optimisation
Using ECGI techniques to reconstruct epicardial isochronal maps, it has been shown that, despite the positive haemodynamic response during LV pacing, only biventricular pacing has resulted in reduced electrical dyssynchrony, represented by decreased total RV and LV activation time.15 The individual configuration of LV quadripolar leads guided by the parameters total ventricular activation time (TVaT) and the time for the bulk of ventricular activation (VaT10–90), which were obtained from ECGI, significantly increased the resynchronisation effect in both ischaemic and non-ischaemic patients.18 The aforementioned parameters, TVaT and VaT10–90, were also used to identify the optimal atrioventricular delay (AVD) and interventricular pacing interval (VVD). The minimum TVaT and VaT10–90 values were associated with the most improved ventricular haemodynamics, suggesting that ECG mapping approaches are effective for programming optimisation.19 The potential of ECGI activation maps for detection of the best configuration of multi-polar pacing was demonstrated in a pilot study with five patients.26
Discussion
One of the therapeutic options for advanced management of HFrEF patients during the last 30 years has been CRT. To increase the efficiency of CRT, different approaches have been applied, such as clinical and experimental approaches, and computer simulation. The experimental porcine model of LBBB to induce electrical and mechanical dyssynchrony was suggested for the study of the mechanisms of CRT effect in a treatment of HF.35 Preclinical studies, including both animal experimental models and patient-specific computational models of the heart, demonstrate a high potential for prediction and optimisation of CRT treatment. Nevertheless, clinical studies are required to validate the efficacy of these models in the target HF population, as well as the applicability of these models to the ECGI methods discussed in this work.36
BSPM could be useful for the selection of HFrEF patients with a borderline QRS width on standard ECG. Most of the evidence suggests that SDAT ≥35 ms from BSPM with 53 leads can predict reverse LV remodelling after CRT, as can the greater change of SDAT (∆SDAT) from baseline to post-implant values. ECGI can further improve patient selection with the use of parameters such as ADV or VEU. BSPM has been advocated as an alternative guide for the positioning of the LV lead during the implant procedure. It is based on the presumption that choosing the pacing site with the greatest reduction in SDAT will correspond to an improvement in haemodynamics as evaluated using invasive measurement of acute haemodynamic response. However, there is no comparison between these BSPM-derived parameters and the simple strategy, such as the selection of the pacing site based on the identification of the late local activation in sinus rhythm. In our opinion, BSPM has a large potential for individualising the optimisation of CRT device programming. This conclusion is based on studies showing that the optimised SDAT parameter is predictive of reverse remodelling, regardless of the baseline characteristics of the CRT candidates.
As an alternative to BSPM, a novel approach based on ultra-high-frequency ECG was recently suggested to improve patient selection for CRT treatment. Jurak et al. demonstrated that an ultra-high-frequency 14-lead ECG technique could improve the application of CRT based on new ECG indices of ventricular depolarisation.37 This technique may prove to be a valuable addition to the discussed BSPM and ECGI methods.
Artificial intelligence techniques have recently been proposed as a promising tool in cardiac electrophysiology to increase the diagnostic accuracy and treatment capabilities of medical technologies such as surface ECG, intracardiac mapping and cardiac implantable electronic devices.38,39 A machine learning model with nine variables demonstrated improved CRT response prediction compared with guidelines.40 Kalscheur et al. developed a random forest model that predicted all-cause mortality and HF hospitalisation in patients receiving CRT implantation, based on pre-implant characteristics.41 Hu et al. successfully applied machine learning techniques with natural language processing to identify a subgroup of patients who were unlikely to benefit from CRT.42 Machine learning models that relied on pre-implantation clinical, echocardiographic, and ECG characteristics produced understandably better predictions of CRT benefit than those that relied on ECG parameters.41,42 This integration approach based on analysis of many clinical parameters may provide a new opportunity for personalised management of patients with HF. The combination of ECGI-derived parameters and machine learning models may provide a pathophysiological interpretation of related clinical features and CRT response.
An advantage of ECGI methods relates to the ability to obtain important information on CRT effect through an electrical solution to a mechanical problem. A solid understanding of the electromechanical structure of the heart is required. Future ECGI developments should therefore aim to increase the modelling capabilities used in ECG technology to reduce the number of required ECG leads, preferably to the standard 12-lead ECG configuration. Recent developments in the anatomical localisation of premature ventricular contractions from a 12-lead ECG using ECGI technology show that the potential of the ECGI technology has not been fully explored.43
Conclusion
BSPM and ECGI can be used in CRT in several ways. There is a potential for improvement of patient selection for CRT, optimisation of CRT programming and LV lead placement. The most promising parameter (and also the easiest to obtain) is SDAT derived from BSPM. Further prospective or randomised trials are necessary to identify the utility of BSPM for routine clinical practice.
Click here to view Supplementary Material.
Clinical Perspective
- For clinical use, the standard deviation of activation times appears to be the most promising parameter for individualised optimisation of CRT device programming without the need for imaging studies.
- Further prospective or randomised trials are necessary to verify the utility of body surface potential mapping for routine clinical practice.
- ECG imaging approaches can provide detailed information on the depolarisation process in ventricles with heart failure, which is crucial for understanding the relationship between electromechanical status and CRT effect.