








Although atrial fibrillation (AF) is considered the most common arrhythmia in clinical practice, its prevalence is relatively low in the young and middle-aged, ranging from 0.5 % in men below 40 years to 1 % by 60 years.1,2 Regular exercise is proposed as a powerful tool for the primary and secondary prevention of cardiovascular disease, reducing most of the risk factors that predispose to AF, such as hypertension, diabetes mellitus, coronary artery disease and obesity.3,4 However, there is growing evidence that long-term endurance exercise may increase the risk of developing AF, with a reported 2–10 times greater prevalence in athletes and those who are involved in long-term sport participation.5
Why athletes should be susceptible to AF is an issue of ongoing debate. Several mechanisms underlying the association between exercise and AF have been proposed but they remain speculative. It is of interest that adaptations such as sinus bradycardia and atrioventricular node disturbances, which are generally considered benign and reversible after a short period of detraining, have been considered by some investigators as a reason for AF development in elderly athletes.6 It is clear that AF in athletes has some differencesin cause, clinical presentation and treatment strategies compared with the general population.7
The aim of this short review is to present the existing data about the epidemiology of AF in athletes and those engaged in long-term endurance sport practice, to analyse the pathophysiological mechanisms that connect AF with exercise, and finally to discuss the existing treatment options.
Prevalence and Incidence of Atrial Fibrillationin Endurance Sport Practice and in Vigorous Physical Activity
The prevalence of AF in the athletic community varies considerably dependent on the age and the number of years of training of thesubjects. It is essential to make a distinction between studies including young athletes with only a few years of training and those with middle-aged or older individuals practising sports for many years. Whereas the incidence of AF in young athletes appears similar to that observed in the general population, in older athletes an increased incidence of AF is reported.6,8–15
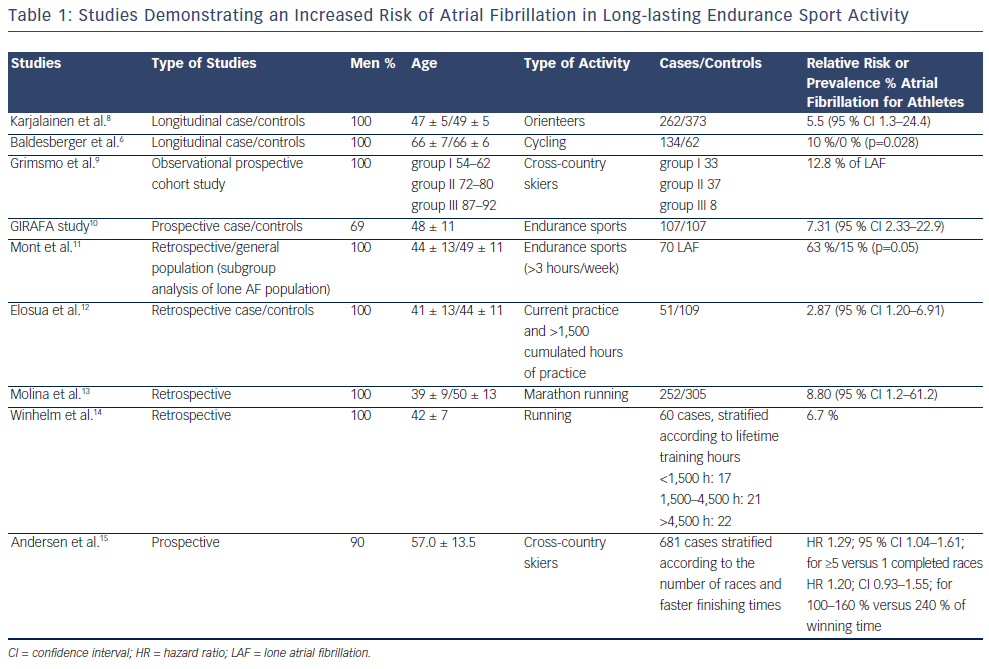
Furlanello et al.16 and Pelliccia et al.17 reported a low rate of AF (0.2 % and 0.3 %, respectively), no different from that observed in the general population. However, both studies included exclusively young athletes with relatively fewer years of training. In contrast, several other studies of middle-aged athletes, who were engaged in sport training for many years, demonstrated an increased prevalence of AF compared with the rest of the population (see Table 1). A common characteristic among all these studies was that the participating athletes were predominately male and they were involved in endurance sports. The prevailing pattern of AF was the so-called vagal lone AF, as it was usually encountered in relatively young individuals (<60 years old) without clinical or echocardiographic evidence of cardiopulmonary disease, and appeared predominantly in vagal circumstances, such as the postprandial period.18 Atrial flutter (AFL) was also frequently reported, implying that endurance sport may contribute to the development of both arrhythmias.6,19
Karjalainen and colleagues8 were the first to establish a relationship between endurance sport practice and AF, reporting a 5.5 odds ratio for AF associated with vigorous exercise, in a series of middle-aged endurance cross-country runners. Elousa et al.12 showed analogous results, with three times higher prevalence of lone AF and five times higher prevalence of vagal AF, indicating a threshold limit of 1,500 lifetime hours of intense endurance practice in order to attain this association. A following meta-analysis of six case-control studies including 655 athletes and 895 controls verified the aforementioned increased overall risk of AF for athletes compared with controls, demonstrating a high odds ratio of 5.29.5
Other studies with longer follow-up not only confirmed the association between endurance sport practice and AF but revealed an even higher prevalence, suggesting that the incidence of AF further increases with ageing in athletes. Indeed, Grimsmo et al.9 showed a 12.8 % prevalence of lone AF after 28–30 years of follow-up in a prospective study of high-performance male participants in endurance cross-country ski competitions, while Baldesberger et al.6 reported a 10 % versus 0 % prevalence of AF and AFL in a comparison of former professional cyclists (mean age 66 ± 7 years) with a control group of male golfers who had never performed high-endurance training. A less pronounced incidence of AF (hazard ratio [HR] 1.29) was reported in a recent large prospective study following athletes who completed long-distance cross-country ski races over a period of 10 years. Nevertheless, the incidence of AF and AFL remained higher in the older group of athletes (55–64 years old).15
According to some reports, not only athletic activity but also vigorous physical activity associated with occupational activities may pose a similar risk for AF. The Girafa study10 showed that the moderate and heavy physical activity, whether sport or jobrelated, increased the risk of AF. Aizer et al.,20 in line with the previous study, found that middle-aged subjects who took moderate exercise (5–7 times a week) had a significant risk (relative risk 1.53, 95 % confidence interval [CI] 1.12–2.09) for developing AF at three-year follow-up compared with controls. On the other hand, the Cardiovascular Health Study,21 which investigated the association between habitual physical activity and AF among 5,446 adults ≥65 years of age over a 12-year period showed that, unlike high intensity exercise, light to moderate physical activity is associated with a lower incidence of AF. A recent meta-analysis,22 including 95,526 subjects, confirmed that regular physical activity is not associated with a higher risk of AF compared with sedentary lifestyle, providing additional strength to the already known beneficial effects of regular exercise on cardiovascular risks.4,23
The concept of a U-shaped pattern relationship between exercise dose and relative risk of developing AF may better explain these apparently contradictory data. According to this theory, regular mild to moderate exercise21,22 may provide a degree of protection from AF, while more sustained vigorous exertion could promote AF.10,15,20 In summary, previous studies indicate a higher incidence of AF among athletes and former competitive athletes compared with the general population. However, this occurs predominately in middle-aged athletes engaged in sport activities over a long time period, which supports the concept that years of endurance training may be necessary before the development of AF. The lack of prospective studies where the exercise dose was accurately measured and the athletes were followed over many years does not allow at present the establishment of a threshold of lifetime hours of sport practice for AF development.
Pathophysiology of Atrial Fibrillation in Athletes
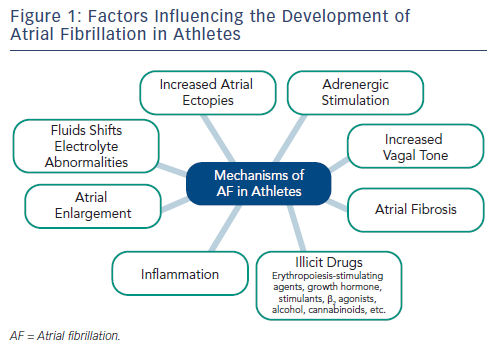
A multifactorial mechanism concerning the role of intense and long-term exercise in the development of AF has been proposed (see Figure 1). Atrial anatomic adaptations due to chronic volume or pressure overload, alterations in autonomic nervous system, chronic systemic inflammation and fibrosis have been suggested as potential mechanisms. However, all these associations still remain speculative.24,25 Fluid shifts and electrolyte abnormalities occurring during vigorous exercise may also trigger AF,26 whereas the use of illicit drugs may be associated with the arrhythmia.27 Nevertheless, it is essential in the work-up of the arrhythmia to exclude any underlying structural (hypertension, cardiomyopathy, myocarditis) or electrical (Wolff-Parkinson-White syndrome [WPW], concealed pathways, channelopathies) substrate for AF as well as extracardiac causes like thyrotoxicosis, as a considerable percentage of athletes with AF may have underlying pathologies.
Atrial Anatomic Adaptation
Even though AF in athletes is considered predominately lone,10,12 evidence of atrium structural alterations, such as enlarged left atrial dimension,17 put this definition into question, raising additional concerns as to whether exercise-induced atrial remodelling is necessarily a benign adaptation to exercise conditioning.
Endurance exercise training is associated with increased left and right atrial size, probably due to long-standing volume and/or pressure overload. Although these conditions can precipitate AF, either by shortening atrial effective refractory period28 and/or eliciting more atrial ectopics, this has yet to be proved in clinical studies. Indeed, Pelliccia et al.17 showed that athletes involved in regular endurance practice have a larger atrium when compared with sedentary controls without this increased size predisposing per se to AF. Furthermore, Baldesberger et al.6 did not find an increased prevalence of atrial ectopy in former professional cyclists in contrast with older studies connecting atrial ectopic activity and physical activity.29
The concept of atrium fibrosis as consequence of long-term intensive exercise training derives exclusively from animal models, while data from athletes’ hearts are non-existent. An increase in mRNA and protein expression of a series of fibrotic markers in the right ventricle and both atria was found in rats exercised for 16 weeks compared with sedentary rats.30 In contrast, histological remodelling in athletes’ ventricles was reported by few clinical studies supporting the concept of fibrosis in humans following long-term engagement in exercise.31,32
Inflammation
The hypothesis that inflammation may play a significant role for AF in athletes derives from many studies that have demonstrated an increase in inflammatory markers such as cytokines interleukin 1 (IL-1), IL-6 and C-reactive protein (CRP) in response to intensive or prolonged endurance exercise.25,33,34 The relationship between elevated inflammatory markers and the risk for developing AF has also been proved.35,36 Nonetheless, this concept remains speculative since no data concerning the association between exercise intensity, amount of inflammation and risk for AF in athletes exist so far.
Autonomic Nervous System
Vagal AF is the prevailing type of AF in athletes.10 A recent study confirmed the relationship between increased vagal tone and AF in middle-aged healthy men.37 The hyperactivity of vagal tone in athletes acting synergistically with a high level of sympathetic activation during training, produce significant shortening of atrial refractory period and increase dispersion of repolarisation, creating the proper conditions for initiation and perpetuation of AF.38–41
Management of Atrial Fibrillation in Athletes
The natural course of AF has not been well-documented in athletes. A study by Hoogsteen et al. showed that lone AF did not demonstrate a severe evolution and is well-tolerated in most athletes.42 It is also essential, before proceeding to specific therapies for AF, to exclude and treat appropriately other possible causes of the arrhythmia, such as hyperthyroidism, myocarditis, pericarditis, WPW syndrome, channelopathies and hypertrophic cardiomyopathy, as well as alcohol consumption and use of illicit sympathomimetic substances.
Although few data support the concept that limitation of sports activities can have favourable outcomes in athletes with AF,16,42 it is advisable to look for cases where arrhythmia may be a manifestation of excessive engagement in sports training. In these cases, a period of detraining for three months to achieve and maintain sinus rhythm is advocated, while the degree of improvement during this resting period will determine whether athletes are allowed to resume their training.43
Pharmacological Therapy
Few data on pharmacological treatment for athletes with AF are available. Even though antiarrhythmic agents used to treat AF in athletes are no different than those used in non-athletes, some issues need specific attention. Beta-blockers, further to their limited efficacy in preventing AF recurrences, are often not well tolerated due to the prevalence of increased vagal tone among athletes.
Another limitation to the use of beta-blockers is their inclusion in the World Anti-Doping Agency prohibited list for specific sports.44 Class IC antiarrhythmic agents, and in particular flecainide, may be useful in preventing AF. However, concomitant use of beta-blocker or calcium channel antagonists is strongly recommended due to the risk of 1:1 conduction to the ventricles if AFL occurs under conditions of sympathetic overactivation. The ‘pill in the pocket’ approach with IC drugs45 may be suitable in some athletes. Sport cessation should be considered for as long as the arrhythmia persists, and until one or two half-lives of the antiarrhythmic drug used have elapsed, according to the current guidelines (Class IIA,C).46 Amiodarone, while being efficient, is not recommended due to its side-effects. Dronedarone has yet to prove its efficacy in athletes.
Pulmonary Vein Ablation
Radiofrequency (RF) ablation of AF emerges as a particularly attractive option for athletes with AF, who would otherwise face a lifetime need for medical therapy, possibly interfering with exercise eligibility or tolerance, aside from the documented proarrhythmic tendency of most of them. The interaction between high levels of sympathetic and parasympathetic activity, increased pulmonary vein (PV) ectopic activity and atrial remodelling in trained athletes comprise a milieu that is highly conducive to promotion of AF. This may render AF more refractory to ablation or it may demand a more extensive approach involving also the ganglionated plexi,47–49 given the pivotal role of the autonomic system in the mechanism of AF in this specific population.
There are few data confirming the efficacy of catheter ablation in athletes. Furlanello et al.50 described a highly successful ablation procedure of PV isolation, with 90 % success after a mean of two ablation procedures in a series of 20 symptomatic elite athletes. Calvo et al.51 reported high efficacy of circumferential PV isolation in endurance athletes with lone AF, proving also that the probability in athletes of remaining free of AF recurrences after a single procedure was similar to the general population. Finally, Koopman et al.52 showed in a series of 59 endurance athletes suffering from paroxysmal focally induced AF, that PV isolation was as effective in athletes as in other patients after three years follow-up. The aforementioned studies, although not allowing for clear conclusions to be made (due to the small number of subjects and the relatively limited follow-up period), suggest that exercise continuation does not appear to act as a trigger for AF evolution after PV isolation. According to the current guidelines, AF ablation in athletes is a Class IIA with level of evidence C indication, which should be considered to prevent recurrent AF when appropriate.46
Cavotricuspid Isthmus Ablation
Long-term endurance exercise may cause right ventricle enlargement usually in parallel with left ventricle dilatation aiming to augment cardiac output and meet the increased metabolic demands during rigorous activity. This remodelling process occasionally leads to structural alterations facilitating electrical instability as well as initiation and maintenance of macro re-entry tachycardias such as typical AFL.53,54 Cavotricuspid isthmus ablation should be considered as first-line therapy in this case, given its high success rate and low incidence of complications.55 According to the recent guidelines, isthmus ablation is a Class IIA-C indication, especially when therapy with flecainide or propafenone is intended.46 A history of endurance sports has been identified as an independent predictor of AF development after AFL ablation, while the continuation of endurance sports activity after ablation showed a trend for increased risk of developing AF.19
Anticoagulation
Indications for oral anticoagulation are the same as in non-athletes. Since most treated athletes present a zero CHADS2 score, aspirin or no-drug can be prescribed.46 Anticoagulation therapy excludes these individuals from participation in close contact sports.
Sports Eligibility
Athletes with asymptomatic AF in the absence of structural heart disease who have an appropriate ventricular response to exercise are eligible for all types of competitive sports. In the presence of structural heart disease, participation in competitive sports should be consistent with the limitations imposed by their disease.56–58 A three-month interruption of sports participation, from the time when stable sinus rhythm was restored, is recommended for athletes with paroxysmal, persistent or even first-onset AF, providing that no major cardiac disease exists. Finally, athletes without structural heart disease whose arrhythmia was eliminated by means of ablation may resume all sports activity at least three months after the procedure, provided that there are no subsequent recurrences. It is essential, however, that these athletes are followed up closely (i.e. every six months).43
Conclusions
There is growing evidence that long-term endurance exercise may increase the risk of AF. However, the bulk of reported data supports the concept that years of endurance training may be necessary before this arrhythmia occurs. Several proposed factors contributing to the mechanism of AF in athletes, such as atrial dilatation, increased atrial ectopic activity, inflammatory changes, fibrosis, and above all the strong influence of vagal tone, remain unproven. Treatment of AF in athletes can be challenging because of limitations in the usage of common antiarrhythmic agents and also due to the lack of randomised studies from which clear guidelines may be produced. Pulmonary vein ablation represents an attractive therapeutic option yet few data are available. Finally, further studies on the intensity and duration of exercise are needed in order to clarify whether a threshold limit for AF development exists.