








The first day’s final session put front and centre a debate that addresses an important clinical economical issue: can we discharge our AF ablation patient the same day instead of keeping him or her overnight?
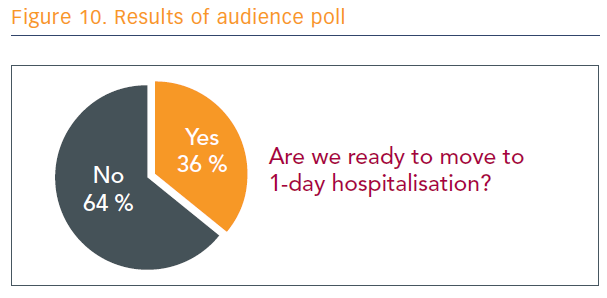
The debate opened by asking the audience to use their interactive, hand-held devices and respond to the question: ‘Are we ready to move to 1-day hospitalisation?’ (see Figure 10).
Protagonist
Reasons for staying in hospital include rest and recuperation, the need for supportive therapy not available at home (e.g. IV pain relief, fluid), monitoring for serious complications, and cardiac rhythm monitoring. However, argues Prof Richard Schilling from Barts Heart Centre London, UK, this kind of support is rarely needed in some patients. For these appropriately selected patients, with the right planning, sameday discharge should become the norm.
Same-day discharge will help make AF more cost-effective and, therefore, more accessible. The median cost of AF ablation is $20,600 in the US, with the most expensive procedures costing more than $77,000.40 Analysis of US data has shown outcomes are not associated with cost and, in fact, the less-expensive procedures tend to be safer.40 Thus, for patients with limited lesions in the left atrium, same-day discharge could be employed to free up resources to be reinvested in more complex patients.
The most common serious complications of AF ablation are cardiac tamponade and vascular complications,7 and many other issues that cannot be prevented by keeping patients in overnight. “Monitoring alone isn’t a reason to keep them in,” said Prof Schilling.
In his practice, Prof Schilling selects only the least complicated patients for same-day ablation, and gives them the choice about how they would like to approach their procedures. If the patients are travelling a long distance, they are encouraged to stay in a nearby hotel before and after their procedures. The procedures are performed in a small, local hospital catheterisation lab by operators trained in a standardised method, using standardised equipment.
The observed 4.8 % complication rate with same-day AF ablation comprises five phrenic nerve palsies (1.9 %), two tamponades (0.7 %), three groin complications (1.1 %), two pericardial effusion with no drainage (0.7 %), and one temporary wire (0.4 %). At 3-month follow-up 58.0 % of patients had complete resolution, 30.4 % had improvement in their conditions, and 19.6 % requested repeat procedures for ongoing symptoms.
“It’s not suitable for everyone, but day-case AF ablation is feasible for some patients,” said Prof Schilling. “It has significantly impacted our waiting times and ability to treat these patients earlier, and earlier AF ablation may result in better outcomes.”
Antagonist
Dr Helmut Pürerfellner from Linz, Austria, acknowledged that sameday AF ablation would be inherently less expensive, and it would be useful to free up money to take care of more patients. However, there is no good clinical data for same-day AF ablation, as it is being performed only in a limited capacity in a few countries, including Canada, the US, the UK and Switzerland. Furthermore, there is no support from any guidelines for same-day ablation, and there are “too many and too-complex potential risks”, especially those that are often delayed, including:
- bleeding (vascular access);
- tamponade;
- transient ischaemic attack/stroke;
- congestive heart failure;
- pericardial chest pain;
- nausea/vomiting;
- migraine;
- phrenic nerve palsy; and
- gastroparesis.
There could also be recurrent arrhythmias, including atrial tachycardia/ AF, inappropriate sinus tachycardia, and sick sinus syndrome with bradycardia or pauses. The human factor, too, should not be discounted, for answering questions, providing reassurance and comfort, enhancing patient satisfaction and ensuring physician satisfaction.
“Seeing how my patient is faring the next day is something I need as a person and a physician,” said Dr Pürerfellner. “Should we adopt same-day discharge as standard clinical practice for AF ablation? In short, no.”
The follow-up audience vote was 31 % yes, 69 % no.